
The Vaccine Dilemma
The Vaccine Dilemma: Systemic Vulnerabilities vs. Public Health Frameworks
This document outlines the core structural arguments driving the modern debate over public health mandates, data integrity, and regulatory oversight. It contrasts the critical perspective—which argues that institutional capture and flawed metrics invalidate the ethical basis for mandates—with the foundational public health framework.
1. The Conflict of Interest Loop
[Pharmaceutical Industry Revenue]
│
├──► Funding via User Fees (approx. 45-65% of FDA drug budgets)
│ └──► Regulatory Capture of Approval Agencies
│
└──► Direct Insurance & Quality Bonuses to Clinics
└──► Physician Quotas (Financial incentive to maximize uptake)
- The Critical View: Regulatory agencies are financially dependent on the industry they oversee through "user fees," creating an inherent conflict. Simultaneously, frontline doctors receive financial bonuses from insurers for hitting high vaccination percentages, incentivizing compliance over independent safety verification.
- The Public Health Framework: User fees accelerate review times for life-saving medications, while physician performance metrics ensure high population immunity against preventable outbreaks. This creates a conflict of interest where a physician is PAID money to ensure he/she gaslights the patients.
2. The Post-Market Surveillance Gap
[Adverse Event Occurs] ──► [Passive Reporting System (VAERS)] ──► [Broken Metric]
▲
No Penalties for Failure to Log
- The Critical View: Passive monitoring systems like VAERS are fundamentally broken. Federal studies (e.g., the 2010 Lazarus/Harvard Pilgrim Report) indicate severe underreporting, estimating less than 1% of adverse events are captured. Because doctors face no legal or financial penalties for failing to report, the "harm data" is systematically missing.
- The Public Health Framework: VAERS is designed as an early-warning signal detection system. Real-world safety is verified by active, large-scale systems like the Vaccine Safety Datalink (VSD), which analyzes electronic health records across millions of patients. The two systems are not related and only VAERS has the legal mandate and is less than 1% updated. The argument collapses.
3. Data Asymmetry in Risk Assessment
[Disease Mortality] ──► Broad Medical Coding Protocols ──► [Inflated Threat Data]
[Vaccine Injury] ──► Passive/Unenforced Reporting ──► [Deflated Harm Data]
│
[Flawed Cost-Benefit]
- The Critical View: The mathematical calculation used to justify mass interventions is structurally manipulated. Threat data from natural diseases is artificially inflated through broad medical coding protocols on death certificates (e.g., classifying dying with a pathogen as dying from it). Conversely, harm data from the intervention is suppressed, rendering a true ethical cost-benefit analysis impossible.
- The Public Health Framework: International coding standards (ICD codes) are required to track infectious trends accurately. Historical and modern epidemiological data consistently show that the morbidity and mortality risks of natural infections far outweigh the documented risks of vaccination. That calls into question the motive of these standards when they gloss over the absence of the post-market harm data.
4. Ethical Collapse of the Harm Principle
[Flawed Safety Data] + [Coercive Policies] ──► Eradication of Informed Consent
- The Critical View: The utilitarian "Harm Principle" states individual liberty can be limited to protect others. However, if the underlying safety data is compromised, the true risk cannot be calculated. Forcing or coercing a procedure under these conditions eliminates the legal and ethical foundation of informed consent.
- The Public Health Framework: Individual bodily autonomy must be balanced against collective biosecurity. When highly contagious diseases threaten vulnerable populations (the elderly, infants, and the immunocompromised), society has a valid ethical obligation to implement proportional mandates to protect public welfare. However, there is a much GREATER concern when the harm data from vaccines is hidden, manipulated and riddled with conflicts of interest.
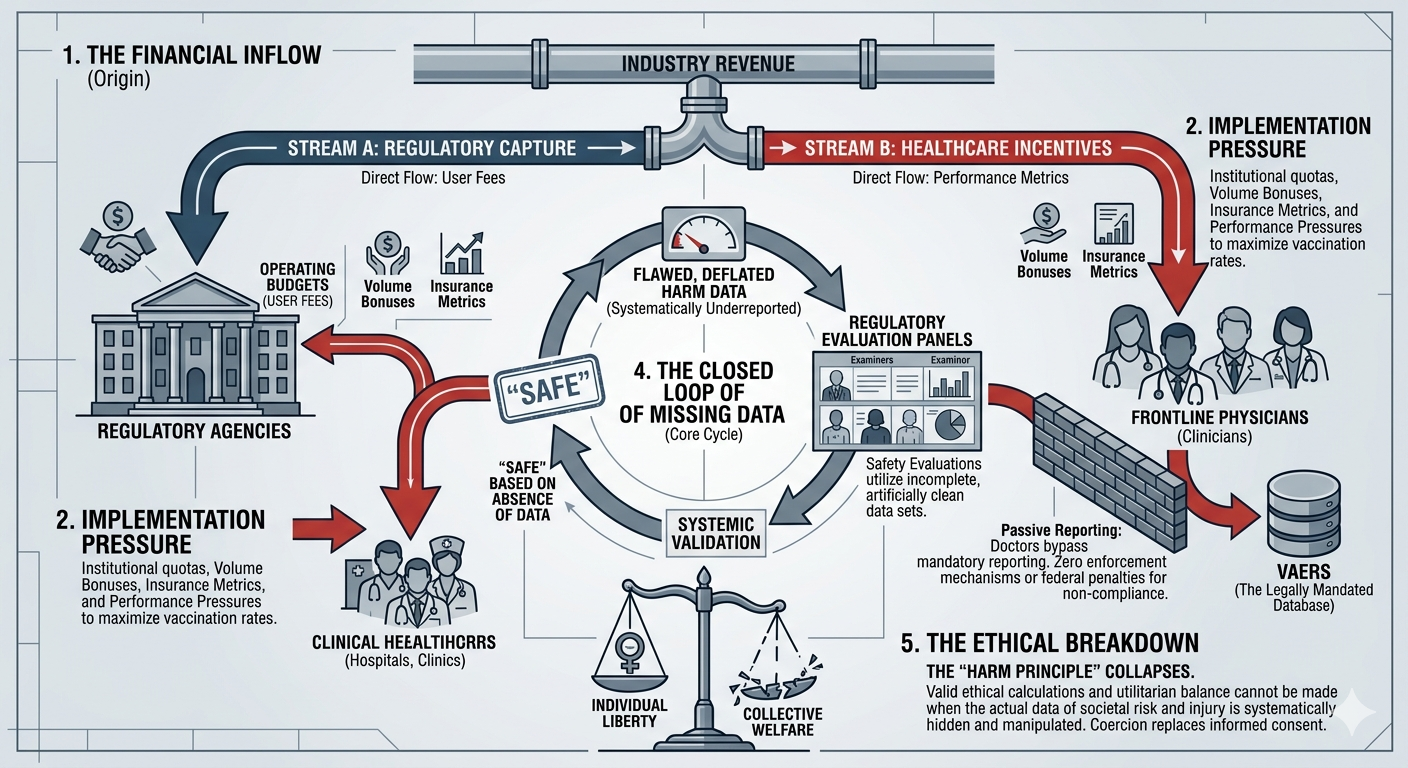
The Closed Loop
This maps out visually, into a single, high-impact flow diagram or quadrant map.
┌─────────────────────────────────────────┐
│ THE CLOSED-LOOP VACCINE DILEMMA │
└────────────────────┬────────────────────┘
│
┌───────────────────────┴───────────────────────┐
▼ ▼
┌──────────────────────┐ ┌──────────────────────┐
│ FINANCIAL CAPTURE │ │ DATA ASYMMETRY │
├──────────────────────┤ ├──────────────────────┤
│ • Pharma funds FDA │ │ • Disease deaths │
│ via user fees. │ │ over-coded. │
│ • Clinics paid for │ │ • Adverse events │
│ high volume. │ │ under-reported. │
└───────────┬──────────┘ └───────────┬──────────┘
│ │
└───────────────────────┬───────────────────────┘
│
▼
┌──────────────────────┐
│ ETHICAL COLLAPSE │
├──────────────────────┤
│ • Harm Principle │
│ built on bad data. │
│ • Coercion replaces │
│ Informed Consent. │
└──────────────────────┘